
Table of Contents
Project Overview: Hospital Sound Masking and HCAHPS Study
- Project: 24-Hour ICU Sound Study with HCAHPS Impact Analysis
- Location: New Orleans, LA — Ochsner Medical Center West Tower
- Facility Type: 7th-Floor Neuroscience ICU, Pre-Move Baseline
- Client: Ochsner Medical Center, Architects on Their Behalf
- Method: Class 1 SPL Meter, 24-Hour Logged Data, 6 Staff Interviews
- Scope: Noise Event Logging, HCAHPS-Aligned Mitigation Plan, Sound Masking
Why HCAHPS Drives Hospital Sound Investment
HCAHPS — the federal Hospital Consumer Assessment of Healthcare Providers and Systems survey — is the reason most hospital sound projects get funded. The survey includes a “quietness of the hospital environment at night” question, and that single line item ties patient noise complaints directly to CMS reimbursement under the Value-Based Purchasing program. A hospital that loses ground on the quietness question loses real money, and facility teams know it.
Ochsner Medical Center brought us into the West Tower expansion as part of their Post Occupancy Evaluation program, the kind of evidence-led work a hospital acoustic consultant brings to clinical environments. The work was a 24-hour sound study of a Neuroscience ICU on the 7th floor before the unit moved to its new home on the 9th floor — a baseline measurement that would let the architects and the operations team compare against the new space a year later. The HCAHPS quietness measure sat in the background of every recommendation we made.

24-Hour Sound Study Method
- Meter: Class 1 Sound Pressure Level meter, calibrated
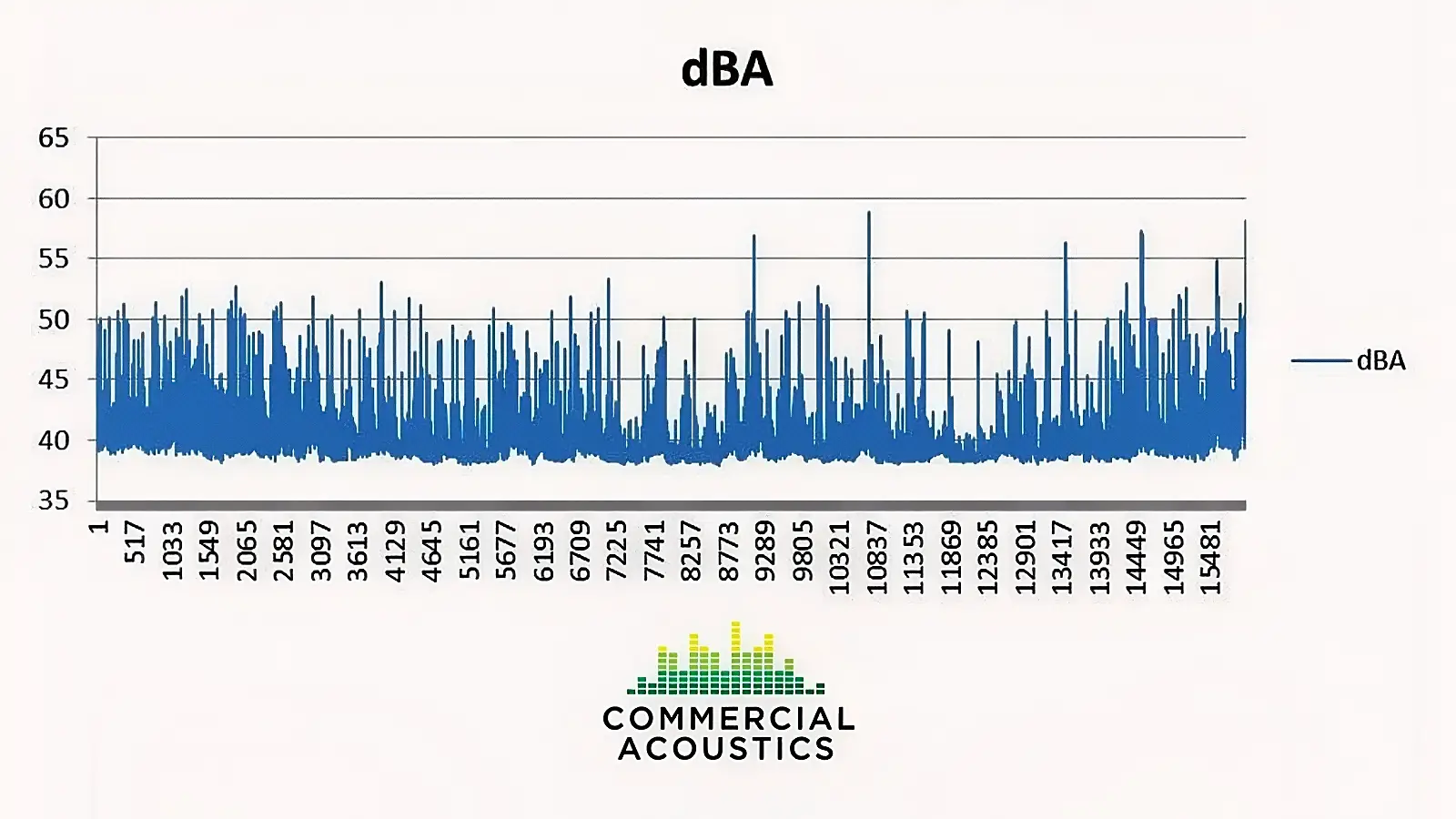
- Logging: 24-hour continuous data in a mock patient room
- Spot Tests: Nurse stations, corridors, equipment rooms
- Qualitative: 6 informal interviews with nurses and nursing staff
The 24-hour patient-room logging was the spine of the study. The meter sat in an office adjacent to the central nurse station — close enough to capture the same noise field a real patient would hear, far enough that staff would not adjust their behavior because of an obvious recording device. Every event was time- and spatial-logged, classified by source type, and any anomalies were called out in the notes.
Quantitative data alone misses the story in a hospital. Six informal staff interviews ran alongside the logging, because nurses know exactly which noises wake their patients up — they have been listening to them for years. A combined quantitative + qualitative method is the right shape for any hospital sound study aimed at HCAHPS outcomes. For the deeper math behind dBA targets in occupied spaces, the design for noise criteria guide walks through the relevant NC ranges.
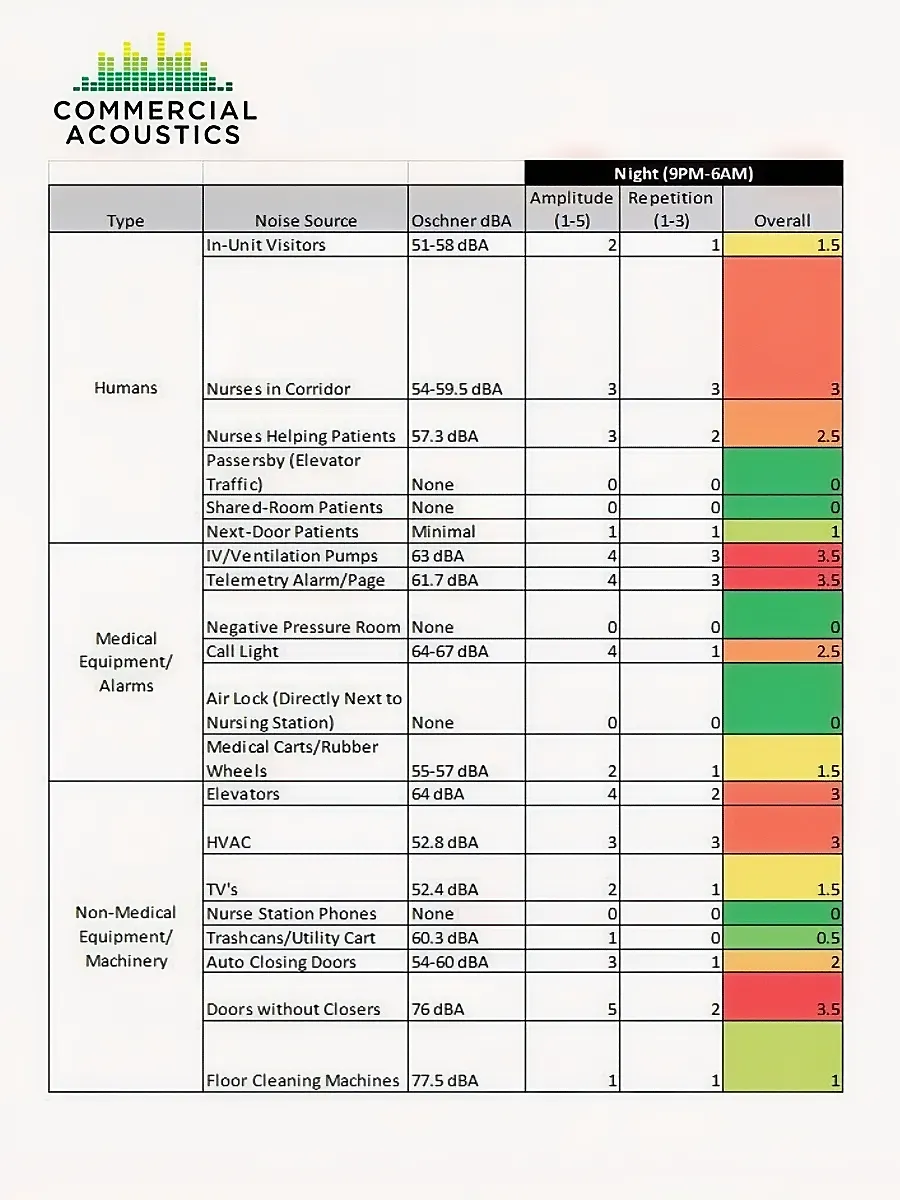
Top Noise Events Disrupting Patient Sleep
- IV Pumps and Telemetry: Alarms held same level overnight as during day
- Staff Conversation: Loud talking and laughter from 9 PM to 1 AM and before 7 AM
- Doors Without Closers: Multiple slamming events overnight
- Policy Gap: No formalized Quiet Hour Policy — staff unaware when quiet hours start
The noise sources ranked highest by the weighting system (amplitude × repetition) were not exotic. They were the standard ICU pattern that NIH and WHO research has flagged for decades. Patient room doors stayed open through both day and night — at 11 AM there were 25 open doors and 9 closed; at 11 PM, 24 open and 10 closed. Lights flipped off at 8:09 PM and back on before 6 AM, neither aligned with the posted Visitation Hours. Overhead pages continued past 9 PM. Music played in the main nursing area at audible volume.
The single biggest underlying issue was the missing Quiet Hour Policy. When nurses do not know when the quiet hours are supposed to start, the unit operates as a 24-hour active environment. Every behavioral noise source — staff voices, music, overhead pages, door management — flows from that one operational gap.
Why Dynamic Range Matters More Than Volume
- Steady 55 dBA: Sleepable for most patients after adjustment
- Fluctuating 40–55 dBA: Wakes patients far more reliably
- Transient Sounds: More disruptive than rhythmic at the same dBA
- Syntax: Names and ringtones cut through where background HVAC does not
The counterintuitive result every hospital sound study lands on: it is not the volume that wakes patients, it is the change in volume. A constant 55 dBA can fade into the background after a few minutes — the brain treats it as noise floor. A fluctuating 40–55 dBA, with sharp transients, never lets the auditory cortex stand down. Patients fall asleep through one and stay awake through the other.
That single insight reframes the whole HCAHPS sound problem. Reducing absolute dBA helps, but reducing dynamic range helps more. Sound masking — the deliberate raising of background noise floor with a controlled, broadband signal — works precisely because it compresses dynamic range. The hallway voices and IV pump alarms become smaller deltas above a slightly higher floor instead of sharp spikes above a quieter one.
Sound Masking and Other HCAHPS-Aligned Mitigations
- Sound Masking: Patient-room broadband masking, addresses receiver side
- Quiet Hour Policy: Formal start/end times, lights/doors/voices specified
- Door Closers: Retrofit every patient and corridor door
- Signage and Tracking: Permanent posters, HCAHPS metrics on monthly reports
The recommendation set spread across both behavioral and physical interventions because that is what actually moves the HCAHPS quietness number. A sound masking system for patient rooms handles the receiver side of the source-path-receiver chain — without it, every other intervention only chips at the edges of the problem. Adding broadband masking to each patient room raises the noise floor by 3 to 6 dB, compresses the dynamic range, and turns sharp hallway events into small ones.
Behavioral interventions are the leverage points the facility team controls. A formal Quiet Hour Policy with named owners at each shift, permanently mounted signage at every entrance, and HCAHPS noise-question scores tracked on monthly management reports together do more than any single physical install. For a sister project that took the sound masking side further with HIPAA-compliance overlap, see the Nova Medical sound masking project.

HCAHPS Scores That Move When Hospital Noise Drops
- Direct: “Quietness of the hospital environment at night” question
- Indirect: Communication, responsiveness, and overall rating questions
- Reimbursement Tie: CMS Value-Based Purchasing Program weighting
- Adjacent: Sleep quality drives recovery time and length-of-stay metrics
The “quietness of the hospital environment at night” question is the obvious target, but the spillover hits other questions on the survey too. Sleep-deprived patients rate communication lower, perceive responsiveness more harshly, and are less likely to recommend the hospital. The published research is consistent on this: better sleep equals better scores across the survey, not just on the quietness line.
For another healthcare project where the operations team paired acoustic intervention with patient-experience tracking, see the Shands Hospital guesthouse soundproofing case study at UF Health Shands. Different facility, different scope, same playbook: measure the noise, fix the operational and physical sources, track what moves on the patient survey.

Conclusion: Hospital Sound Masking and HCAHPS
The Ochsner West Tower 24-hour Neuro ICU sound study mapped exactly which noise events wake patients overnight — IV pump alarms held at daytime levels, staff voices well past 1 AM, slamming doors, an absent Quiet Hour Policy — and tied each one to an intervention that moves the HCAHPS quietness score. Sound masking handles the receiver side; behavioral policy and door hardware handle the source side. Hospital teams that run these studies tend to see the work pay back through both reimbursement and patient outcomes. More on the team that runs hospital sound studies if you are scoping one of your own.
FAQs: Hospital Sound Masking and HCAHPS
What is HCAHPS and why does it matter for hospital noise?
HCAHPS is the federal Hospital Consumer Assessment of Healthcare Providers and Systems survey. It includes a question on the quietness of the hospital environment at night that ties directly to CMS Value-Based Purchasing reimbursement. A hospital that loses ground on the quietness question loses real money, which is why facility teams fund acoustic interventions.
Does sound masking actually move HCAHPS scores?
Yes, when paired with operational fixes. Sound masking compresses the dynamic range patients experience, which matters more than absolute decibel level for sleep quality. The published research is consistent: hospitals that combine masking with a formal Quiet Hour Policy and door-closer retrofits see measurable lifts on the quietness question and adjacent survey measures.
How loud is too loud in a hospital ICU?
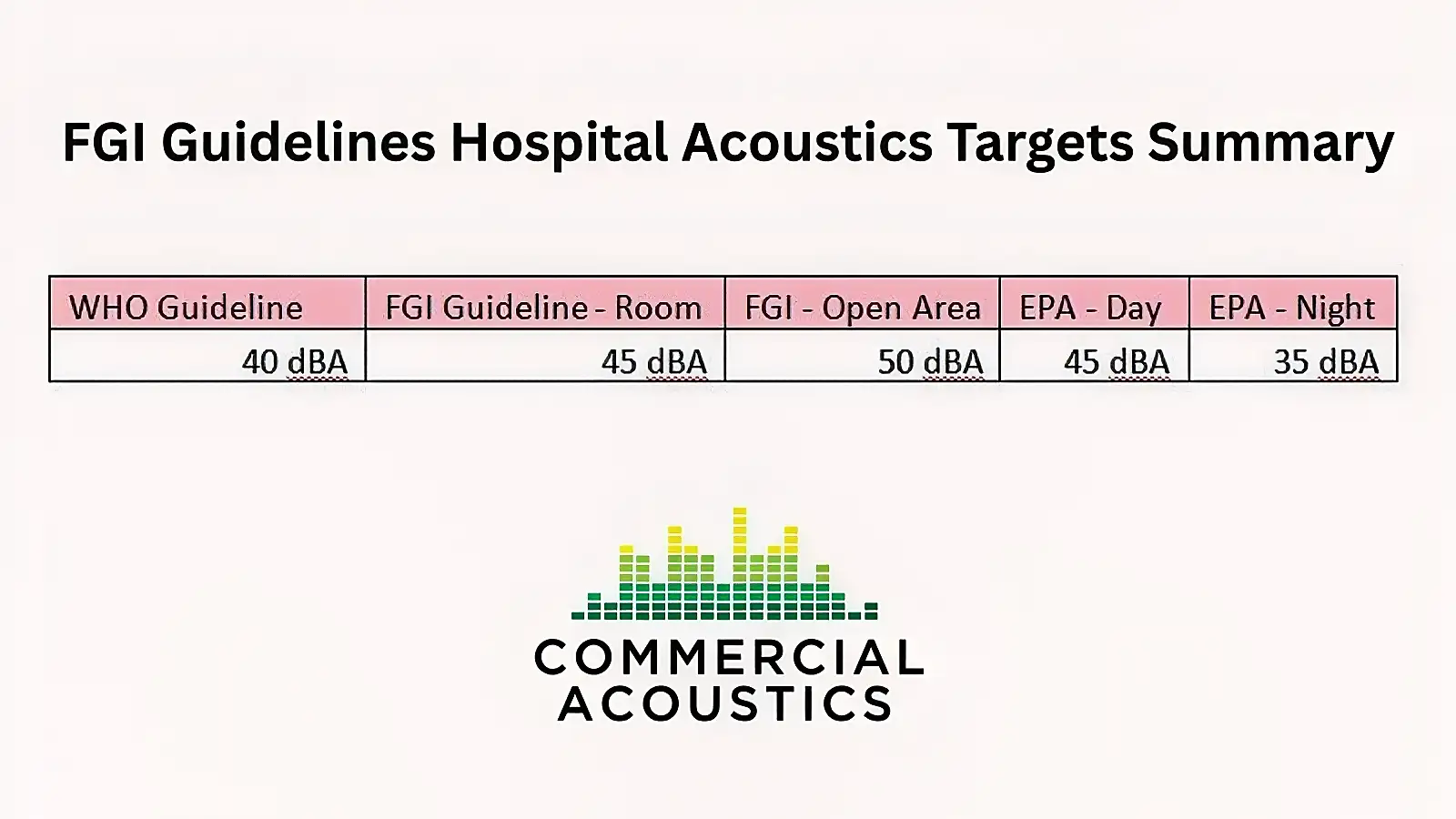
WHO recommends 35 dBA daytime and 30 dBA nighttime for hospital patient rooms. Most ICUs measure well above that — typical baselines run 50 to 65 dBA daytime and 45 to 60 dBA nighttime. The bigger driver of patient sleep disruption is dynamic range rather than absolute level: fluctuating sounds wake patients far more reliably than steady ambient.
How does a 24-hour hospital sound study work?
A Class 1 SPL meter logs continuous data in a mock patient room, with spot tests at nurse stations, corridors, and equipment locations. Staff interviews capture qualitative context the meter misses. The deliverable is a noise event ranking weighted by amplitude and repetition, plus a mitigation plan tied to HCAHPS-aligned outcomes.

Walker Peek|Founder & CEO, Commercial Acoustics
Walker founded Commercial Acoustics in 2013 to bring aerospace-grade engineering discipline to soundproofing, and runs the firm as CEO from its 12,000 sq ft Tampa production facility. The company designs custom acoustic panels, sound membranes, and masking systems for multi-family, hospitality, healthcare, and commercial projects across the US — built around Walker’s invention, Wall Blokker, an EVA-based sound barrier that hits STC 50-plus at roughly $1 per square foot installed.
A Jacksonville native, Walker spent five years at Kennedy Space Center with Craig Technologies before founding Commercial Acoustics — certifying aerospace manufacturing to the AS9100 standard and leading Six Sigma Black Belt process-improvement teams on NASA programs. He is a certified Industrial Noise Control Engineer and the author of Architectural Acoustics: A Practical Handbook.